Pityriasis rubra pilaris (Devergie’s disease) is a rare chronic skin condition in which red or orange-red patches appear with fine scaling and firm papules around hair follicles. The skin may become dry and thickened.
The condition is not contagious and is not transmitted from person to person. It can present in different ways: from small localized patches to widespread skin involvement. In some cases, improvement or complete recovery occurs over time.
This condition is rare, but in most cases it can be managed with proper medical supervision and treatment.
What to do if you suspect it
If you notice red scaly patches, thickened skin, or small firm bumps, it is important not to delay seeing a specialist.
The first step is to consult a dermatologist. The doctor will examine the skin and may order additional tests to confirm the diagnosis and rule out similar conditions.
Additionally:
- do not use strong hormonal medications on your own
- avoid aggressive cosmetic procedures
- monitor changes in the rash
It is important not to self-treat. Incorrect treatment can alter the appearance of the disease and make diagnosis more difficult. Without treatment, the condition may gradually spread and cause significant discomfort.
How the disease looks
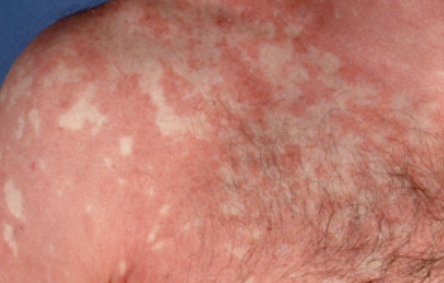
The disease presents with red skin areas with characteristic fine scaling.
Typically observed:
- red or orange-red patches and plaques
- dry “powder-like” scaling
- small firm papules around hair follicles (felt as skin roughness)
- thickening of the skin on palms and soles
A characteristic feature is the presence of “islands” of healthy skin within affected areas.
Most commonly affected areas:
- trunk
- arms and legs
- scalp
- palms and soles
Lesions may gradually enlarge and spread. Presentation varies widely—from limited patches to almost complete skin involvement.
Below in the article you can view real photos to better understand how the condition looks.
Main symptoms
Symptoms may develop gradually and worsen over time.
Most typical:
- skin redness
- scaling
- dryness and tightness of the skin
- skin thickening (especially on palms and soles)
- mild itching (not in all patients)
In some cases, the condition can cause significant cosmetic and physical discomfort.
Causes of the disease
The exact cause is not fully known.
It is thought that important factors include:
- immune system dysregulation in the skin
- inflammatory processes
- genetic predisposition (rare cases)
It is important to understand that this is not an infection — it is not caused by bacteria or fungi and is not contagious.
How the disease develops
There is a disruption in the normal process of skin cell turnover. Cells regenerate faster than usual and do not mature properly.
This leads to:
- accumulation of scales
- thickening of the skin
- redness and inflammation
Around hair follicles, firm papules form, making the skin feel rough.
Forms and types
The disease can present in different ways:
- localized form — limited areas of skin involvement
- generalized form — large areas of the body are affected
There are also age-related variants (childhood and adult forms), which may differ in course.
When to see a doctor
See a specialist if:
- the rash is spreading or becoming more pronounced
- there is significant skin thickening
- there is marked itching or discomfort
- there is uncertainty about the diagnosis
It is also important to seek medical advice if treatment is ineffective or the condition worsens.
Treatment
Treatment depends on severity and is selected individually.
Main approaches:
- skin care and moisturization
- reduction of inflammation with topical treatments
- management of excessive skin thickening
In more severe cases, systemic medications may be used to affect skin processes from within.
Also important:
- regular use of emollients
- avoiding irritants
- keeping the skin well hydrated
Treatment should be carried out under medical supervision.
Questions and answers
Can this disease be cured?
In many patients, improvement or complete recovery occurs over time, although it may take months or years.
Is it contagious?
No, the disease is not transmitted from person to person.
Do I need to take tablets?
Sometimes yes — in widespread cases, a doctor may prescribe systemic therapy.
Is this disease dangerous?
Usually not, but it can significantly affect quality of life when symptoms are severe.
Why does the skin become thick?
This is due to accelerated skin cell turnover and accumulation on the surface.
Can it go away on its own?
Yes, in some cases symptoms gradually disappear.
Can it be confused with psoriasis?
Yes, the conditions may look similar, so medical diagnosis is important.
Do I need to change my skincare routine?
Yes, gentle and regular skin care helps reduce symptoms.
Check Your Skin Instantly
Use Dermatology scanner app – Skinive AI to take a photo of a skin lesion and get an AI-based risk assessment. It helps determine whether professional consultation is recommended, giving you fast guidance and peace of mind.
Medical sources used
- Fitzpatrick’s Dermatology, 9th Edition
- European Academy of Dermatology and Venereology (EADV) Guidelines
- American Academy of Dermatology (AAD)
- Clinical Dermatology (Bolognia et al.)
🇬🇧 Pityriasis rubra pilaris: Diagnosis and Treatment in the UK
If you notice papulosquamous disorders—conditions that cause raised red bumps and scaling on the skin, such as psoriasis or lichen planus—it’s important to get a professional opinion. In the UK, you can access dermatology care via the NHS, private clinics, or online dermatology consultations.
👉 How to See a Dermatologist in the UK NHS – This main guide explains how NHS referrals work, what to expect from specialist dermatology services, and how to choose between public and private care.
Dermatologists in Major UK Cities:
- Dermatologist in London
- Dermatologist in Manchester
- Dermatologist in Liverpool
- Dermatologist in Birmingham
- Dermatologist in Leeds
- Dermatologists in Other UK cities
Online Dermatology
If you prefer remote care or faster access, try online dermatology consultations. They allow dermatologists to review images, provide advice, and guide next steps without visiting a clinic. Read more in this article: Online Dermatologists in UK.
🇦🇺 Pityriasis rubra pilaris: Diagnosis and Treatment in Australia
If you notice papulosquamous disorders—conditions that cause raised red bumps and scaling on the skin, such as psoriasis or lichen planus, it’s important to get a professional opinion. In Australia, dermatology care is available via Medicare (public system), private clinics, or online consultations.
👉 How to See a Dermatologist in Australia – This main guide explains how referrals work through GPs and public clinics, what to expect from specialist dermatology services, and how to choose between public and private care.
Dermatologists in Major Australian Cities:
- Dermatologist in Sydney
- Dermatologist in Melbourne
- Dermatologist in Brisbane
- Dermatologist in Perth
- Dermatologist in Adelaide
- Dermatologists in other Australian cities
Online Dermatology
For faster access or remote care, online dermatology consultations allow dermatologists to review images, provide advice, and guide next steps without visiting a clinic. Read more in this article: Online Dermatologists in Australia.
Images of Devergie disease:





















** Should you identify any copyright infringement regarding the images on this page, kindly reach out to us at info@skinive.com.
Furthermore, please be advised that these photos are not authorized for any purpose.