A dysplastic nevus is a pigmented skin lesion that may resemble a common mole, but has a more complex structure and a higher risk of developing into melanoma.
These nevi are not contagious, but they require careful monitoring. They can appear at any age and often occur in large numbers, especially in people with sun-sensitive skin.
It is important to understand: this is a benign lesion, but with potential risk, so it should be treated more cautiously than ordinary moles.
What to do if suspected
If you notice an unusual mole — with irregular borders, uneven color, or changes over time — it is important to consult a dermatologist or oncologist as soon as possible.
The doctor will perform an examination and dermatoscopy — a magnified skin inspection that helps assess the structure of the lesion. In some cases, a biopsy or immediate excision followed by histological analysis may be required.
It is difficult to evaluate these nevi on your own, as they can resemble early melanoma.
Important: do not delay medical consultation, do not traumatize the lesion, do not attempt to remove it yourself. Early diagnosis is a key safety factor.
How the disease looks
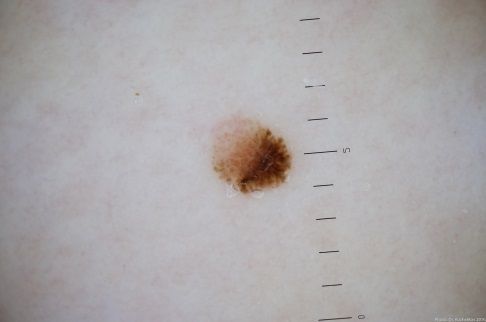
A dysplastic nevus can vary in appearance, but it has characteristic features.
It may appear as a flat or slightly raised lesion, an asymmetrical shape, irregular or indistinct borders.
Color is often uneven: from light brown to dark brown, with areas of pink, red, or even bluish tones.
Sometimes multiple colors are present within a single lesion.
The size is usually larger than common moles — typically up to 1–1.5 cm, but can be larger.
These nevi can occur anywhere on the body.
Below in the article you can view real photos to better understand how the condition looks.
Main symptoms
Most often, a dysplastic nevus does not cause discomfort.
Possible symptoms include mild itching (especially after irritation or sun exposure).
The main signs are related to appearance: asymmetry, uneven color, irregular borders.
Causes of the disease
The exact cause of dysplastic nevi is unknown, but several factors increase the risk of their development.
External factors: ultraviolet radiation exposure (sun, tanning beds)
Internal factors: heredity, hormonal changes, individual skin characteristics
Skin trauma and other external influences may also play a role.
How the disease develops
A dysplastic nevus develops from melanocytes — cells that produce skin pigment.
Under various influences, these cells begin to divide unevenly, forming a lesion with irregular structure and pigmentation.
These changes are benign, but over time may transform into melanoma, especially with sun exposure or repeated trauma.
Forms and types
Dysplastic nevi may differ in size, shape, and degree of atypical features.
They may be single, but are more often multiple.
For the patient, the most important factor is not the subtype, but regular monitoring and follow-up.
When to see a doctor
You should consult a doctor if the nevus starts growing, its color changes or becomes uneven, borders become irregular or blurred, itching, pain, or bleeding appears, or the lesion has been injured.
Regular skin checks are also recommended if you have multiple such nevi.
Treatment
Dysplastic nevi are often removed because they can be difficult to distinguish from early melanoma.
The main treatment is surgical excision followed by histological examination. This allows for a definitive diagnosis.
Destructive methods (such as laser or cryotherapy) are not used, because tissue must be preserved for analysis.
In some cases, observation may be possible, but only under medical supervision and if there are no signs of change.
Treatment is individualized, and regular monitoring is essential.
Q&A
Is a dysplastic nevus dangerous?
It is considered a lesion with an increased risk of developing into melanoma, so it requires monitoring or removal.
Does a dysplastic nevus need to be removed?
Often yes, especially if there are changes or diagnostic uncertainty. The decision is made by a doctor.
How is a dysplastic nevus treated?
The main method is surgical removal followed by histological examination.
How is it different from a common mole?
It more often has irregular borders, uneven color, and variable shape.
Is it already cancer?
No, but it is a condition with increased risk of developing cancer.
Can I tan if I have such nevi?
Not recommended — it is important to protect the skin from ultraviolet exposure.
Can it be observed without removal?
Sometimes yes, but only under medical supervision and if stable.
What if there are many of them?
Regular dermatological check-ups are required to monitor changes.
Check Your Skin Instantly
Use the Skin cancer detector: Skinive AI to take a photo of a mole or lesion and get an AI-based risk assessment. It helps determine whether professional consultation is recommended, giving you fast guidance and peace of mind.
Medical sources
- Fitzpatrick’s Dermatology
- World Health Organization (WHO) Classification of Skin Tumours
- American Academy of Dermatology (AAD)
- DermNet NZ
- UpToDate
🇬🇧 Dysplastic Nevus: Assessment and Care in the UK
If you notice an unusual skin lesion, it’s important to get a professional opinion at your earliest. In the UK, you can access dermatology care via the NHS, private clinics, or online consultations.
👉 How to See a Dermatologist in the UK NHS – This main guide explains how NHS referrals work, what to expect from specialist dermatology services, and how to choose between public and private care.
Dermatologists in Major UK Cities:
- Dermatologist in London
- Dermatologist in Manchester
- Dermatologist in Liverpool
- Dermatologist in Birmingham
- Dermatologist in Leeds
- Dermatologists in Other UK cities
Online Dermatology
If you prefer remote care or faster access, try online dermatology consultations. They allow dermatologists to review images, provide advice, and guide next steps without visiting a clinic. Read more in this article: Online Dermatologists in UK.
🇦🇺 Dysplastic Nevus: Assessment and Care in Australia
If you notice borderline or precancerous skin lesions, it’s important to get a professional opinion. In Australia, you can access dermatology care via Medicare (public system), private clinics, or online consultations.
👉 How to See a Dermatologist in Australia – This main guide explains how referrals work through GPs and public clinics, what to expect from specialist dermatology services, and how to choose between public and private care.
Dermatologists in Major Australian Cities:
- Dermatologist in Sydney
- Dermatologist in Melbourne
- Dermatologist in Brisbane
- Dermatologist in Perth
- Dermatologist in Adelaide
- Dermatologists in other Australian cities
Online Dermatology
For faster access or remote care, online dermatology consultations allow dermatologists to review images, provide advice, and guide next steps without visiting a clinic. Read more in this article: Online Dermatologists in Australia.
Images of dysplastic nevus:
























** Should you identify any copyright infringement regarding the images on this page, kindly reach out to us at info@skinive.com.
Furthermore, please be advised that these photos are not authorized for any purpose.