Lentigo-melanoma is a malignant skin tumor that develops from pigment-producing cells (melanocytes). It most often arises from an existing pigmented spot and appears on skin that has been exposed to long-term sun damage, especially on the face.
It is a type of melanoma. In early stages it grows slowly, but if it progresses it can spread to other organs. Therefore, early detection is crucial. The condition is not contagious.
It most commonly occurs in people over 50 years old. With timely treatment, the prognosis is significantly better than in late stages.
What to do if suspected
If you notice changes in a pigmented spot or the appearance of a suspicious new lesion, it is important to see a doctor as soon as possible.
The first step is consultation with a dermatologist or oncologist. The doctor will perform an examination, dermoscopy (magnified skin inspection), and if necessary will recommend removal or biopsy for an accurate diagnosis.
Additionally:
- any change in color, shape, or size is a reason for medical evaluation
- if the spot becomes uneven or starts bleeding — do not delay the visit
It is important not to attempt removal or use “home” treatments.
Early consultation significantly improves treatment outcomes and reduces complications.
How the disease looks
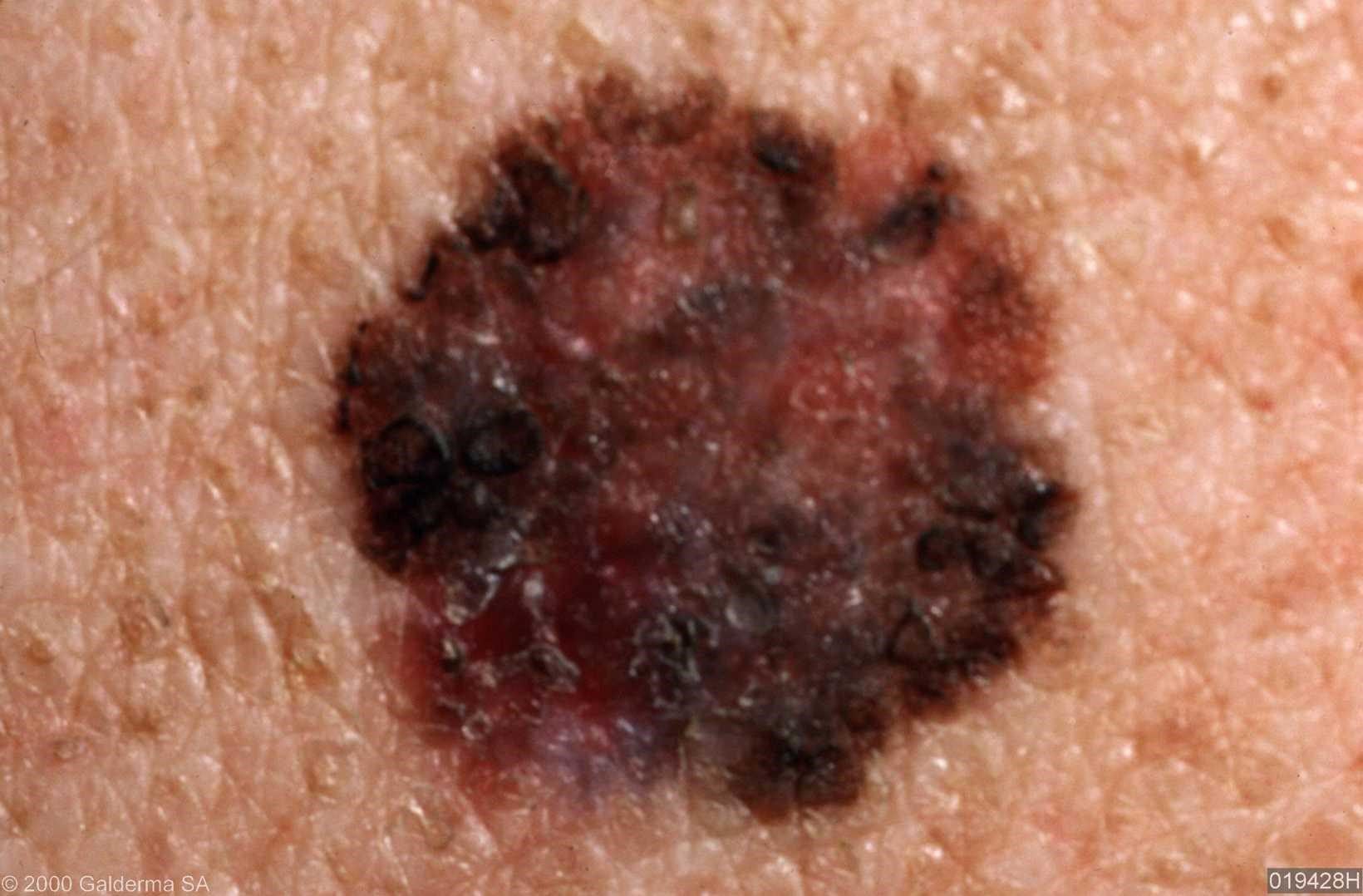
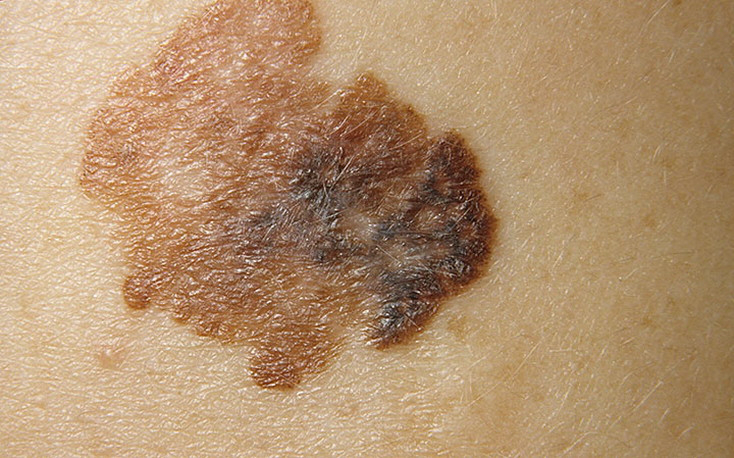
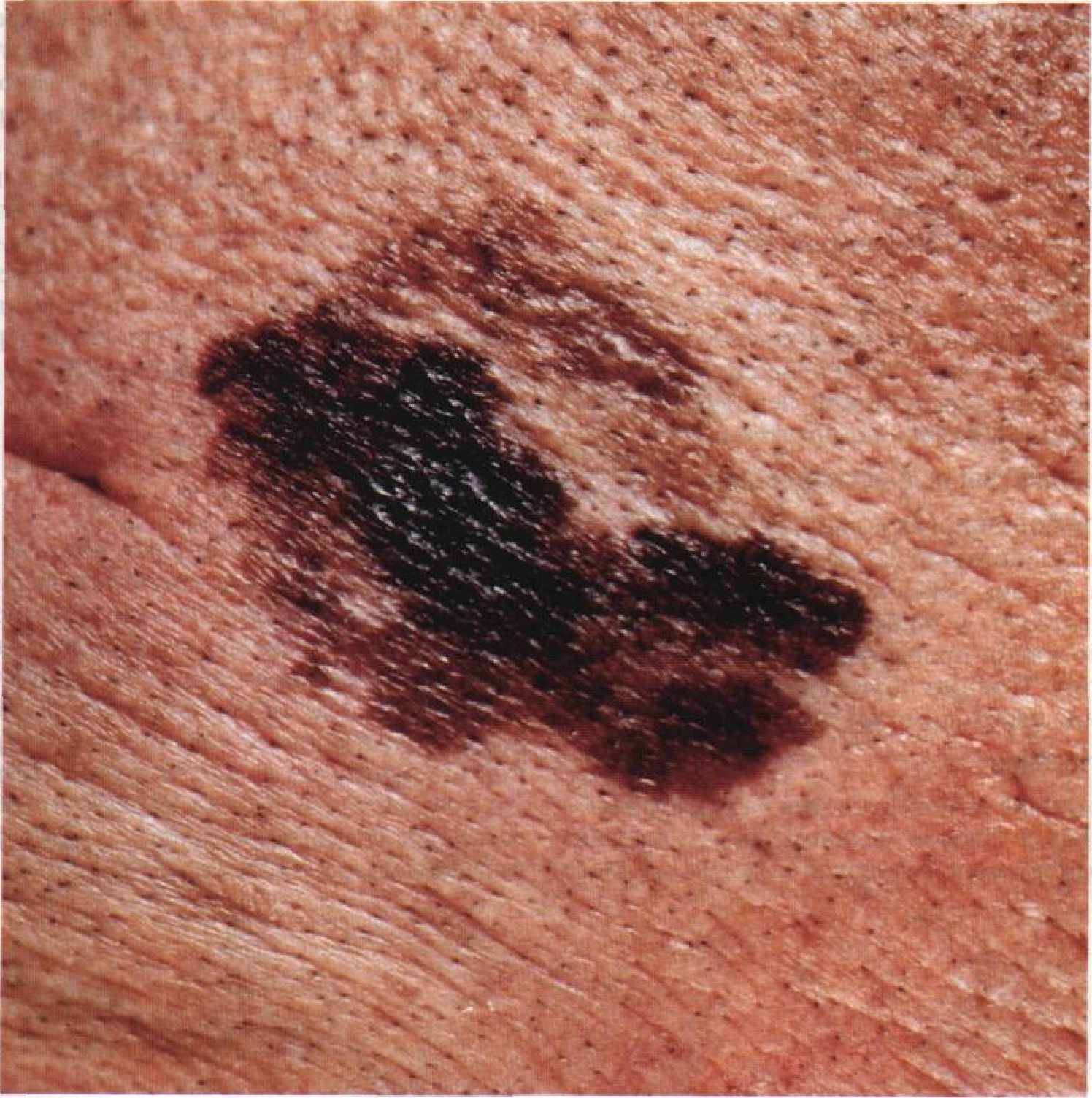
Lentigo-melanoma usually appears as a pigmented patch with irregular features.
Main signs:
- asymmetrical shape
- irregular, “blurred” borders
- uneven pigmentation
The color may include:
- light and dark brown shades
- black
- sometimes blue, pink, or even whitish areas
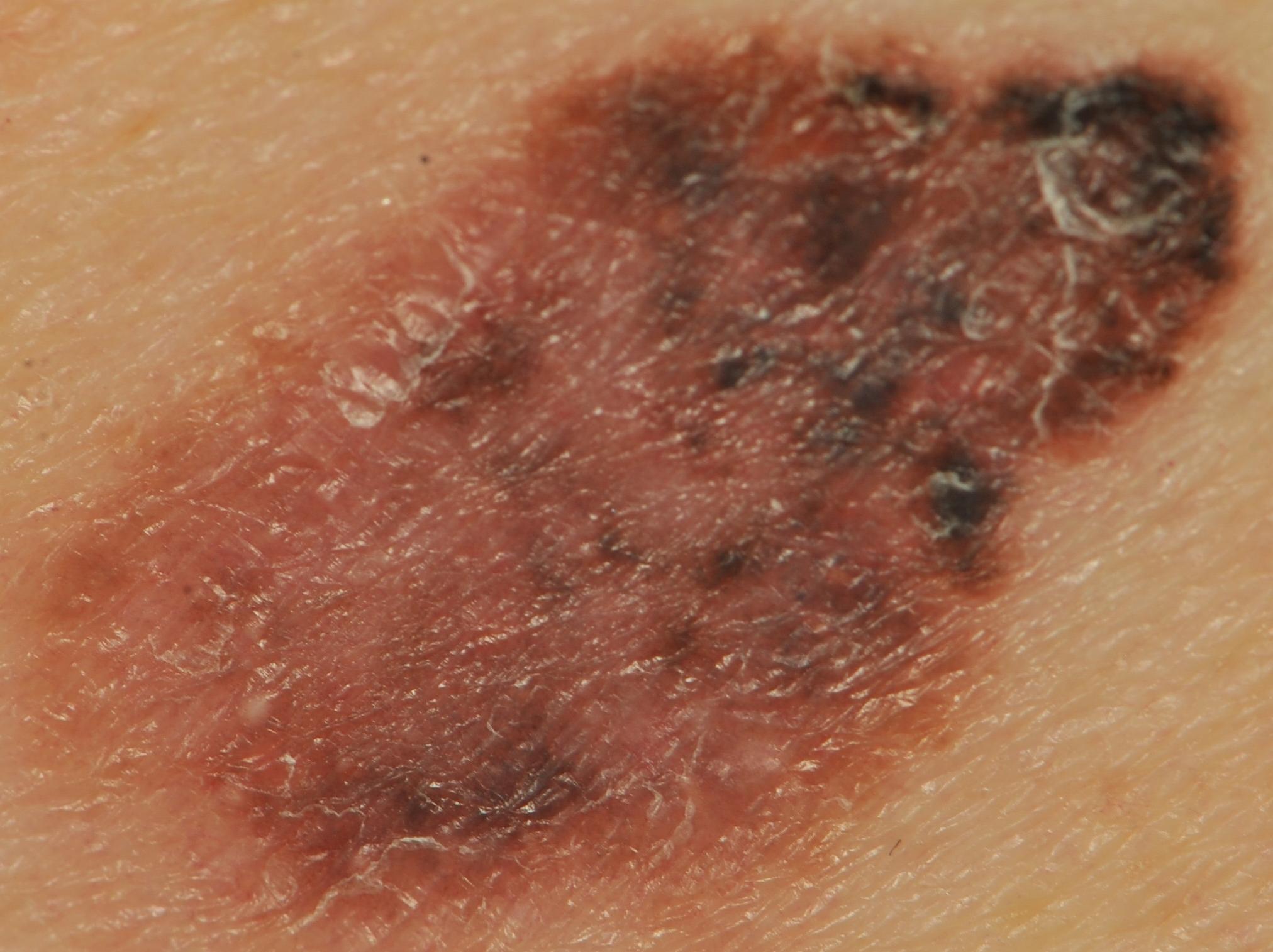
Over time, it may develop:
- thickening
- raised or bumpy surface
- ulceration or bleeding
In early stages it tends to grow slowly in width, but later it may grow deeper into the skin.
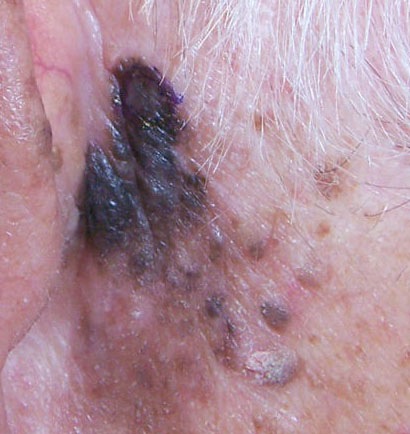
The most common location is the face and other sun-exposed areas.
Below in the article you can see real photos to better understand what the condition looks like.
Main symptoms
In early stages, symptoms may be minimal.
Things to watch for:
- change in shape of a pigmented spot
- asymmetry
- uneven coloration
- gradual increase in size
Also possible:
- itching or tingling
- loss of hair within the lesion
- formation of crusts or bleeding
A helpful guideline is the ABCDE rule:
- asymmetry
- irregular borders
- multiple colors
- diameter larger than ~5–6 mm
- any change over time
Causes of the disease
Lentigo-melanoma most often develops due to long-term ultraviolet exposure.
Main risk factors:
External:
- sun exposure
- tanning beds
- chronic skin damage
Internal:
- fair skin
- light or red hair
- light eyes
- tendency to sunburn
- older age (50+)
- genetic predisposition
A key role is also played by a precancerous condition called Dubreuilh melanosis (a long-standing pigmented patch).
How the disease develops
Lentigo-melanoma begins in the upper layer of the skin.
At first, abnormal cells spread slowly across the surface, sometimes over many years. Later, the tumor may grow deeper into the skin.
In simple terms, early growth is “horizontal”, and later it becomes “vertical”. This transition increases the risk of spread within the body.
Forms and types
Lentigo-melanoma is a distinct type of melanoma.
It may look different depending on the stage:
- early stage — flat pigmented patch
- later stage — thicker lesion with an irregular surface
Appearance can vary significantly between individuals.
When to see a doctor
You should see a specialist if:
- an existing pigmented spot has changed
- a new unusual spot appears
- there is asymmetry, irregular borders, or multiple colors
- bleeding, itching, or thickening occurs
Even one of these signs is a reason for consultation.
Treatment
The main treatment is surgical removal of the tumor.
Additionally, depending on the case:
- wider surgical excision margins
- treatment of lymph nodes (if involved)
- additional therapies (immunotherapy, radiation, or drug therapy)
Treatment depends on the stage of the disease.
Important:
- treatment is always individually selected by a doctor
- surface treatments (laser or cryotherapy) are not suitable
After treatment, regular follow-up is essential.
Q&A
Can lentigo-melanoma be cured?
Yes, if detected early, treatment is often successful.
Is it dangerous?
Yes, it is a malignant tumor that can spread in the body, so timely treatment is essential.
How is lentigo-melanoma treated?
Mainly by surgical removal, sometimes combined with other therapies.
Is it the most dangerous type of skin cancer?
It is one of the more serious types, but early detection greatly improves prognosis.
How fast does it grow?
Often slowly at first, but it may accelerate as it progresses.
Can it be distinguished on your own?
Not reliably. Any suspicion should be checked by a doctor.
Who is at risk?
People with fair skin, frequent sunburns, and long-term sun exposure.
Should moles be checked regularly?
Yes, regular skin checks help detect changes early.
Check Your Skin Instantly
Use the Skin cancer detector: Skinive AI to take a photo of a mole or lesion and get an AI-based risk assessment. It helps determine whether professional consultation is recommended, giving you fast guidance and peace of mind.
Medical sources
- World Health Organization (WHO)
- National Cancer Institute (NCI)
- American Academy of Dermatology (AAD)
- NCCN Clinical Practice Guidelines in Oncology (Melanoma)
🇬🇧 Lentigo melanoma: Diagnosis and Treatment in the UK
If you notice suspicious or skin cancer lesions, such as a new growth, persistent sore, or changes in an existing spot—including a raised bump, ulceration, or slow-healing lesion—it’s important to contact your GP immediately and seek professional care, which in the UK is available via the NHS, private clinics, or online dermatology consultations.
👉 How to See a Dermatologist in the UK NHS – This main guide explains how NHS referrals work, what to expect from specialist dermatology services, and how to choose between public and private care.
Dermatologists in Major UK Cities:
- Dermatologist in London
- Dermatologist in Manchester
- Dermatologist in Liverpool
- Dermatologist in Birmingham
- Dermatologist in Leeds
- Dermatologists in Other UK cities
Online Dermatology
If you prefer remote care or faster access, try online dermatology consultations. They allow dermatologists to review images, provide advice, and guide next steps without visiting a clinic. Read more in this article: Online Dermatologists in UK.
🇦🇺 Lentigo melanoma: Diagnosis and Treatment in Australia
If you notice suspicious or skin cancer lesions, such as a new growth, persistent sore, or changes in an existing spot—including a raised bump, ulceration, or slow-healing lesion—it’s important to contact your GP immediately and seek professional care. In Australia, dermatology care is available via Medicare (public system), private clinics, or online consultations.
👉 How to See a Dermatologist in Australia – This main guide explains how referrals work through GPs and public clinics, what to expect from specialist dermatology services, and how to choose between public and private care.
Dermatologists in Major Australian Cities:
- Dermatologist in Sydney
- Dermatologist in Melbourne
- Dermatologist in Brisbane
- Dermatologist in Perth
- Dermatologist in Adelaide
- Dermatologists in other Australian cities
Online Dermatology
For faster access or remote care, online dermatology consultations allow dermatologists to review images, provide advice, and guide next steps without visiting a clinic. Read more in this article: Online Dermatologists in Australia.
Images of lentigo melanoma:




















** Should you identify any copyright infringement regarding the images on this page, kindly reach out to us at info@skinive.com.
Furthermore, please be advised that these photos are not authorized for any purpose.