Pustular psoriasis is a rare and more severe form of psoriasis in which small pus-filled blisters (pustules) appear on the skin. These usually develop on inflamed, red skin and may be accompanied by pain or tenderness.
A key feature is that these blisters are not caused by infection. They do not contain bacteria; instead, they are filled with immune cells. Therefore, the condition is not contagious and cannot be transmitted through contact.
Pustular psoriasis can vary in severity: in some cases it affects only the palms and soles, while in more severe cases it can involve large areas of the body and significantly affect general health. With appropriate medical care, the condition can often be controlled.
What to do if you suspect it
If you notice painful pustules filled with whitish material, especially on the palms or soles, it is important to see a dermatologist as soon as possible.
The first step is a specialist consultation. A doctor will assess the rash and determine the type of psoriasis.
If high fever, chills, weakness, or rapidly spreading skin lesions occur, urgent medical attention is required. In such cases, hospital treatment may be necessary.
It is important not to self-treat. Incorrect or aggressive treatments can worsen inflammation and skin damage.
How the disease looks
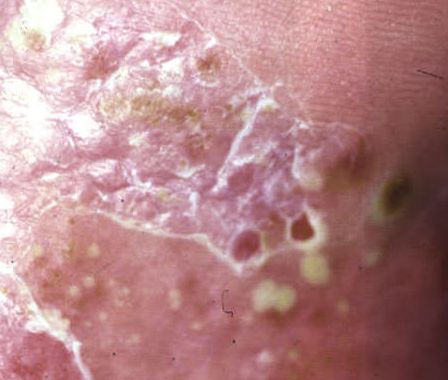
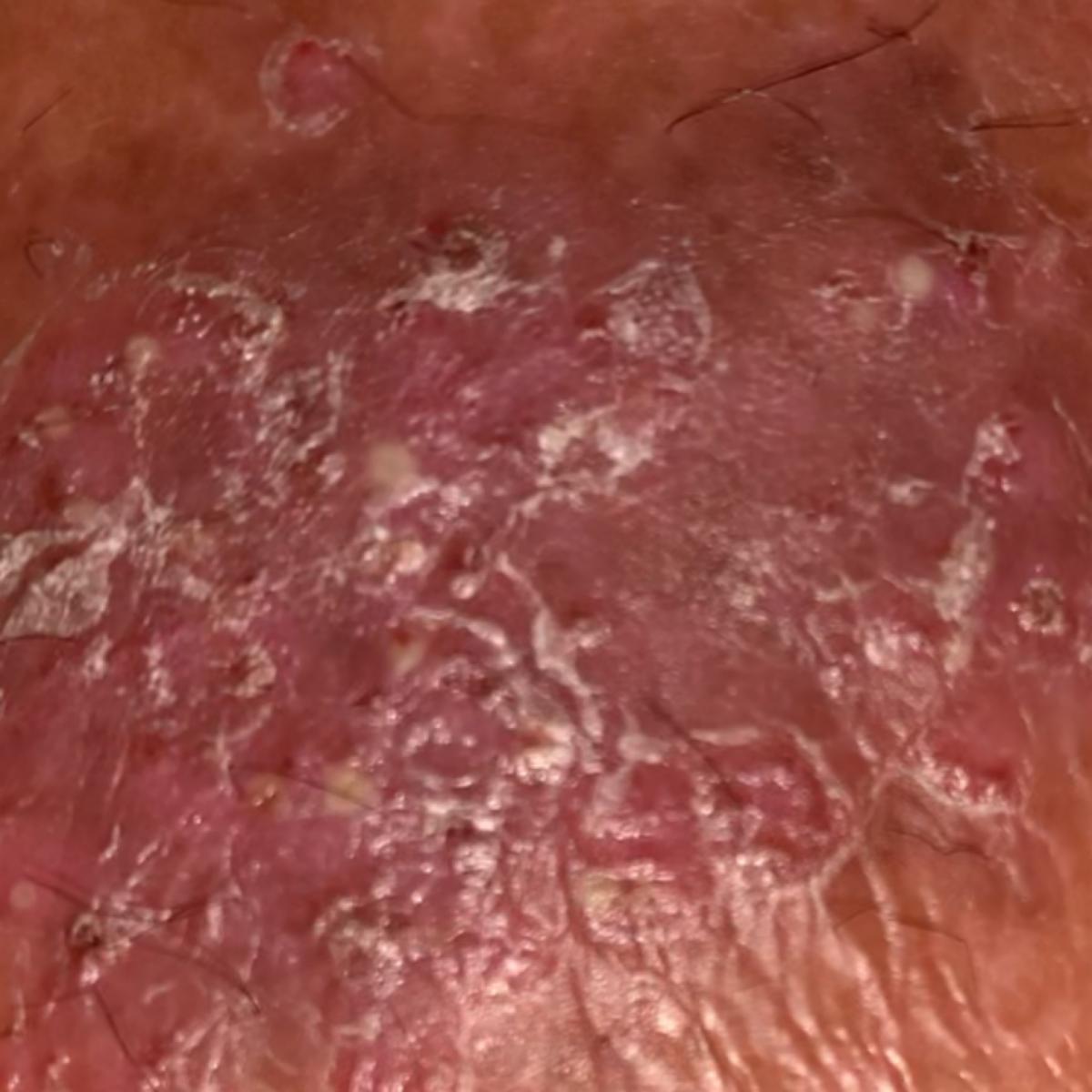
Pustular psoriasis appears as small pus-filled blisters on red, inflamed skin.
In localized forms, the palms and soles are most commonly affected: the skin becomes thick, dry, and painful, often developing cracks.
In generalized forms, pustules may spread over large areas of the body and appear rapidly. After rupturing, they leave crusts and red patches.
The appearance and severity can vary significantly between individuals and may change over time.
Below in the article you can view real photos to better understand how the condition looks.
Main symptoms
The main sign is the presence of multiple pustules on the skin.
Other possible symptoms include:
- pain and burning sensation of the skin
- dryness and cracking, especially on palms and soles
- redness and inflammation
- in severe cases, fever, weakness, and chills
In generalized forms, overall health can be significantly affected.
Causes of the disease
Pustular psoriasis is caused by immune system dysfunction, leading to excessive inflammation in the skin.
Skin cells begin to function abnormally, and immune cells accumulate in the skin, forming pustules.
Contributing factors may include:
- internal factors — genetic predisposition and immune system characteristics
- external triggers that can provoke flare-ups
Important: infection is not the cause of the disease, although infections can sometimes trigger exacerbations.
How the disease develops
The condition is driven by an excessive inflammatory response in the skin.
The immune system becomes overactive and recruits large numbers of immune cells to the skin. These accumulate in the superficial layers and form pustules.
At the same time, the skin barrier is impaired, making the skin more fragile, dry, and sensitive.
Forms and types
Two main forms are distinguished:
- localized form — most often affects palms and soles, with chronic relapsing course
- generalized form — more severe, with widespread lesions and systemic symptoms
When to see a doctor
Seek medical attention if:
- multiple pustules appear on the skin
- lesions are painful or rapidly spreading
- palms or soles develop painful cracks
- fever, weakness, or chills occur
- there is sudden deterioration of condition
Generalized pustular psoriasis requires urgent medical care.
Treatment
Treatment depends on severity and clinical form.
Mild or localized cases are usually treated with topical therapies — creams and ointments that reduce inflammation, soften the skin, and restore barrier function.
More severe cases may require systemic treatments that affect the immune system, as well as phototherapy.
Generalized pustular psoriasis is treated in a hospital setting, where overall health, hydration, and vital parameters are closely monitored.
Treatment is always individualized. It is essential to follow medical instructions carefully and not stop therapy without guidance.
Questions and answers
Is pustular psoriasis dangerous?
Localized forms are usually manageable, but generalized pustular psoriasis can be a serious condition requiring urgent care.
Can it be cured?
It cannot be completely cured, but symptoms can often be controlled with appropriate treatment.
How is it treated?
Treatment may include topical therapies, systemic medications, and hospital care in severe cases.
Is it contagious?
No, it is not contagious and is not caused by infection.
Why do the blisters look like pus?
They are not true pus — they are collections of immune cells involved in inflammation.
Can pustules be popped?
No, this can damage the skin and worsen the condition.
Can stress trigger flare-ups?
Yes, stress is a common triggering factor.
Is a special diet needed?
There is no universal diet, but healthy eating and avoiding harmful habits may help reduce flare-ups.
Check Your Skin Instantly
Use Dermatology scanner app – Skinive AI to take a photo of a skin lesion and get an AI-based risk assessment. It helps determine whether professional consultation is recommended, giving you fast guidance and peace of mind.
Sources
- Clinical guidelines for psoriasis management
- American Academy of Dermatology (AAD)
- European Academy of Dermatology and Venereology (EADV)
- World Health Organization (WHO)
🇬🇧 Pustular psoriasis: Diagnosis and Treatment in the UK
If you notice papulosquamous disorders—conditions that cause raised red bumps and scaling on the skin, such as psoriasis or lichen planus—it’s important to get a professional opinion. In the UK, you can access dermatology care via the NHS, private clinics, or online dermatology consultations.
👉 How to See a Dermatologist in the UK NHS – This main guide explains how NHS referrals work, what to expect from specialist dermatology services, and how to choose between public and private care.
Dermatologists in Major UK Cities:
- Dermatologist in London
- Dermatologist in Manchester
- Dermatologist in Liverpool
- Dermatologist in Birmingham
- Dermatologist in Leeds
- Dermatologists in Other UK cities
Online Dermatology
If you prefer remote care or faster access, try online dermatology consultations. They allow dermatologists to review images, provide advice, and guide next steps without visiting a clinic. Read more in this article: Online Dermatologists in UK.
🇦🇺 Pustular psoriasis: Diagnosis and Treatment in Australia
If you notice papulosquamous disorders—conditions that cause raised red bumps and scaling on the skin, such as psoriasis or lichen planus, it’s important to get a professional opinion. In Australia, dermatology care is available via Medicare (public system), private clinics, or online consultations.
👉 How to See a Dermatologist in Australia – This main guide explains how referrals work through GPs and public clinics, what to expect from specialist dermatology services, and how to choose between public and private care.
Dermatologists in Major Australian Cities:
- Dermatologist in Sydney
- Dermatologist in Melbourne
- Dermatologist in Brisbane
- Dermatologist in Perth
- Dermatologist in Adelaide
- Dermatologists in other Australian cities
Online Dermatology
For faster access or remote care, online dermatology consultations allow dermatologists to review images, provide advice, and guide next steps without visiting a clinic. Read more in this article: Online Dermatologists in Australia.
Images of pustular psoriasis:


























** Should you identify any copyright infringement regarding the images on this page, kindly reach out to us at info@skinive.com.
Furthermore, please be advised that these photos are not authorized for any purpose.